Why I (still) use Polyvagal Theory
Recently there has been some debate about the validity of PVT (Polyvagal Theory) so I wanted to share my thoughts about it and how it impacts my work with clients. Here’s what I’ll discuss:
What is Polyvagal Theory - a very brief outline
What the debate is about - and what isn’t being questioned
Implications for practice - how I am adapting

The vagus nerve
The vagus nerve, aka the ‘wandering nerve’ carries signals to the brain from the digestive system & heart. It’s important for many bodily functions as well as emotional regulation.
What is Polyvagal Theory?
I did my training in PVT in 2020 with co-founder Deb Dana and have been using it in practice ever since. It was created by Steven Porges in 1994 as a way to understand and treat trauma and has since expanded to treat a wide range of conditions such as chronic health problems, anxiety and depression. As I am an integrative counsellor, I use it as part of a toolkit of theories, resources and approaches that I apply depending on the unique needs and nature of the client I’m working with.
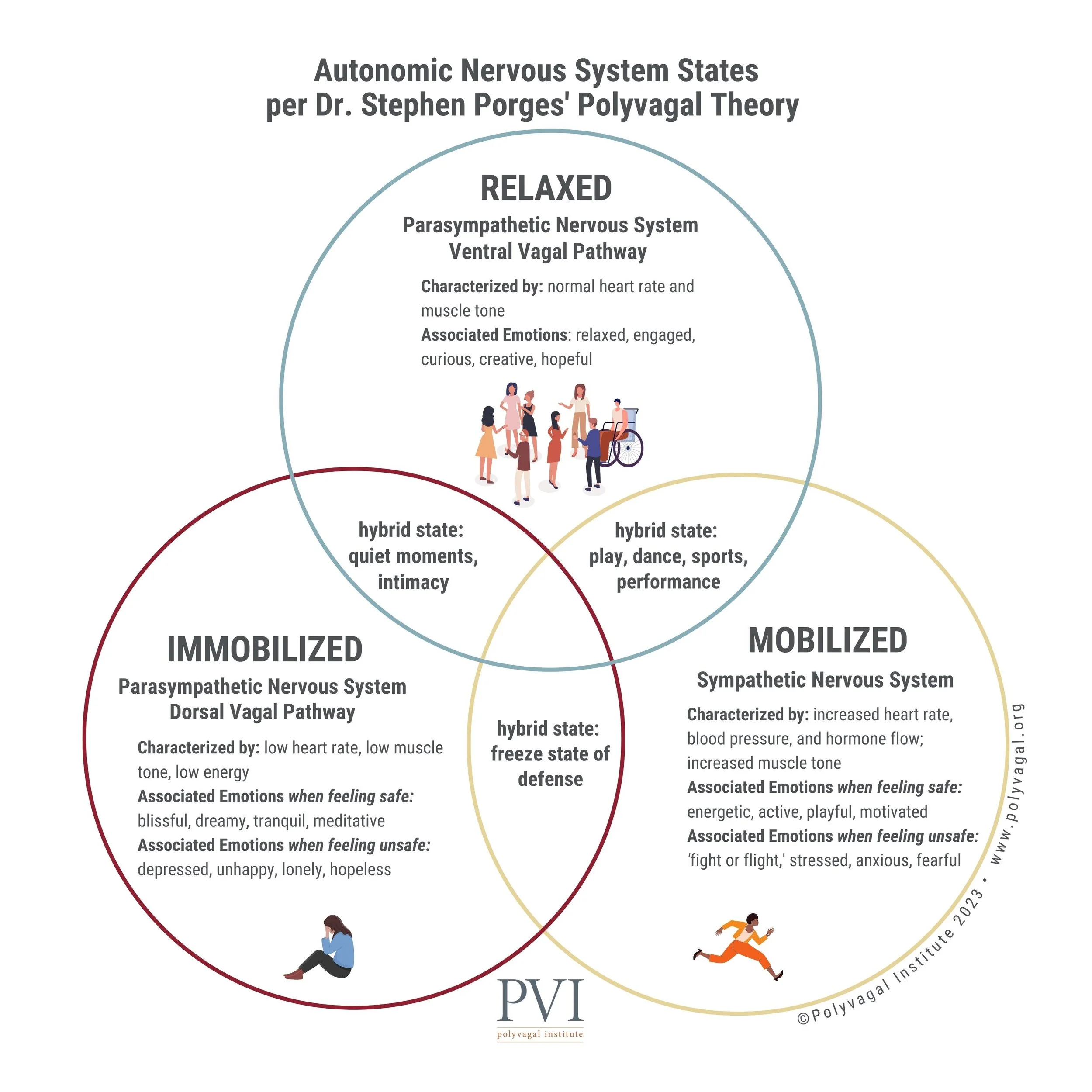
PVT is a model for understanding the autonomic nervous system; describing the different states we can be in and providing a map for how to move between states. The application in clinical practice is about:
helping clients understand why their experiences have impacted them, without the need for going over traumatic events. This is incredibly valuable as it removes shame around automatic reactions and reframes dysregulation as a protective response. Clients learn they are not broken, but have felt threatened and need to find their way back to safety and connection.
in the moment self awareness - using simple language to map where they are on the ANS “ladder” based on their bodily sensation, thoughts, emotions and behaviour. E.g. noticing that I’m becoming snappy with my husband and have tense shoulders tells me I am in a mobilised “fight or flight” state and could do with engaging in some soothing activities to help me re-regulate.
teaching skills to move between states. The goal is never to be regulated 100% of the time as this is totally unrealistic and actually undesirable. The aim is to be in the appropriate state for the situation, and to be able to move back towards regulation after a stressful/dangerous experience.
this translates to spending more time in a regulated state (when not in a situation like being in a war zone and genuinely experiencing threat to life). This is especially important for clients overcoming PTSD and chronic anxiety/depression, but is valuable for everyone from a wellbeing point of view.
Key aspects of PVT that are not controversial
The critique of PVT is about very specific biological aspects of the theory (which I’ll bravely attempt to explain below!) and doesn’t affect the key concepts that practitioners like myself use on a regular basis. The following aspects are widely supported and backed by research.
The vagus nerve plays a crucial role in regulation
Co-regulation is incredibly important - for therapists this is vital aspect of relational therapy
Neuroception - that the nervous system constantly, unconsciously scans the environment for cues of safety and danger. There is some debate about which nerves this is specifically linked to but that level of detail is not relevant in my counselling practice and doesn’t change the validity of neuroception as a concept.
Understanding states such as “freeze” as adaptive, protective responses (as mentioned above this is de-shaming/de-pathologising and therefore very important for recovery).
Techniques for activating the parasympathetic/regulated state such as breathwork, social interaction, vocal cues (e.g. humming), soothing sensory practices etc. These remain well supported common practice for trauma informed therapy.

Co-regulation with nature - tree hugging still very much valid!
PVT RIP?? Regulating myself before responding.
When I first started seeing social media posts titled things like “polyvagal theory is cancelled!” and “RIP PVT”, like many practitioners, I had a momentary panic. But then, ironically (or maybe, fittingly?) I recognised that I had gone into a sympathetic state of dysregulation: mobilisation/fight & flight. I was unsure if I needed to defend the theory (fight) and myself - or drop it completely and distance myself from it (flight). I quickly became overwhelmed and did nothing (dorsal vagal - freeze). I was aware of all this whilst it was happening, and thanks to PVT itself, I was able to notice it and choose how to proceed. I knew not to act from my dysregulated state, that my reaction was a normal stress response to a perceived threat and that I could focus on regulating myself and, in time, responding calmly. I stepped away from the dramatic social media posts and continued to focus on helping my clients, whilst taking care of myself. When I was ready, I researched the debate with the help of resources like Jessica Maguire’s workshop on the current research and various articles by practitioners like myself who have experienced the many benefits of PVT in their practice.

In my nervous system workshop I invite attendees to think of an animal that represents each NS state. My flight response is a panicky pigeon for the chaotic way they flap about.
So what’s the criticism of polyvagal theory?
Honestly, when I discovered what the debate was about I breathed a sigh of relief. The pigeon could stop flapping. Yes, there are certainly aspects that are being rightly debated but my summary - as a counsellor not a neurobiologist - is that the issues are about the detailed biology and not particularly relevant to how it’s used in practice, at least not at the level I work at.
Here’s my basic understanding of the beef with PVT:
The evolutionary hierarchy is incorrect. Porges says that mammals evolved a "new" ventral vagal system (linked to social engagement) that is distinct from an "old" reptilian dorsal vagal system (linked to freeze/shutdown). Evolutionary biologists argue that this is a "profound oversimplification." Research shows that reptiles also have complex vagal structures and social-like behaviors. The "old" and "new" distinction is not supported by modern comparative anatomy; the system is more of an integrated web than a linear ladder of evolutionary progress. (Gemini, March 2026)
Respiratory Sinus Arrhythmia (RSA) is not an accurate measure of vagal tone by itself. Honesty, I hadn’t heard of RSA before researching all this and whilst I fully admit I don’t understand it I can also say that it’s not relevant and I haven't been monitoring client’s heart rates or suggesting they do this themselves. This seems to be more of an issue for researchers choosing methods of showing efficacy than for clinicians.
The dorsal vagal response (freeze) is about more than just the vagus nerve. This surprised me as a criticism because I already assumed it was the case. I knew PVT wasn’t saying only dorsal activation caused freeze and was already aware of how the amygdala plays an important role. The criticism here, as I understand it, is that the model oversimplifies how the nervous system works.

The debate around the evolution of the various states gets pretty deep into evolutionary biology, with scholars arguing about if it’s just mammals that have a social engagement system or if reptiles do too. The fact is that whatever the answer, it changes nothing about the application of PVT in a counselling setting.
Implications for my practice
In short, this changes very little about the way I use polyvagal theory. What I’ve learned from my research into the debate is that I was already blending my understanding of the nervous system with other established models, such as Dan Siegel’s Window Of Tolerance and explaining the concepts to clients at a level that doesn’t touch on evolutionary biology or heart rate variability. I’m glad the scientists are debating these things - I certainly want the work I do to have a solid evidence base. It’s OK for me and my clients that the model is simplified; it gives us a shared language to talk about what is going on in their minds and bodies in the moment. It still provides us with skills for regulating and reinforces the value of co-regulation and social connection.
As mentioned at the start of this article, I work in an integrative way, so I am in no danger of reducing clients to just nervous system states. PVT is a useful framework for understanding physiological responses, noticing stress triggers and learning to find more safety and connection. I will continue to use it, when relevant and appropriate, alongside other theories such as attachment, transactional analysis, compassion focused therapy and humanistic principles.
I had the thought, whilst reading through the criticisms, that perhaps I’ve been using PVT “wrong” this whole time, in a way that’s turned out to actually be “right”. Because I have not really talked very much about the vagus nerve itself - with clients or in my workshop - focusing instead on helping people recognise the different states and their purpose and empowering clients with regulation practices. It’s tempting to claim that this was instinct, or even some kind of unconscious doubt about the more detailed biological aspects of the theory…but it wasn’t. It was a combination of not knowing enough about the neurobiology to attempt to speak about it and knowing that it wasn’t necessary in order to use polyvagal theory to effectively help myself and my clients.

A Labrador is my image for a regulated state - social, playful, intelligent, likes a snooze in front of the fire.
A calm conclusion
I think this is another case of social media taking things out of context and removing nuance. Cancel culture strikes again! If we’re only going to work with theories that have zero criticism then we’re not going to be left with much to work with. The distress many practitioners felt, myself included, when the debates ramped up, was in large part because we feared losing something that we know - irrefutably - has had profoundly positive effects on our clients. Yes, there’s the worry that we’ll look silly or unprofessional if it all turns out to be bunkum (which it isn’t) but more than that - at least I speak for myself here - the concern was deeply protective of the very real healing I have experienced personally and facilitated professionally with many clients. Thankfully, that progress remains unchallenged and unaffected by the neurobiological details that continue to be debated.
“Despite valid neurobiological critiques of the model, we find the polyvagal theory to be a useful paradigm for trauma recovery and psychosomatic healing….. Psychotherapies informed by mind-body integration modalities can facilitate self-regulation and a sense of safety in the world…. Vagal exercises are within everyone’s reach and can easily be taught to our patients, in the office or in group therapy settings. Polyvagal approaches seem cost-effective and there is a plethora of available resources.” - Giroux et al
For more information I recommend reading Porges response to the criticisms made by Grossman and colleagues, referenced below.
References:
Jessica Maguire, Is Polyvagal Theory Evidence Based workshop, 2026
Giroux, Ahlers & Miawotoe in Journal of psychiatry reform, Oct 2023
Polyvagal Institute - critical discussion